Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Sign up
 (044) 394 90 94
(044) 394 90 94
Sign up
(044) 394 90 94
Doctors



 Prices
Blog
Contacts
Prices
Blog
Contacts
пр.Лобановського, 130, Київ, Україна
Temporarily closed
Opening soon
78A, Irpinska St., Kyiv, Ukraine
Temporarily closed
Opening soon
32A, Heroiv Dnipra St., Kyiv, Ukraine
Temporarily closed
Opening soon
9B, Yevhena Chykalenko St. (Pushkinska), Kyiv, Ukraine
Temporarily closed
Opening soon
(044) 394 90 94
Back
Dentistry

General Dentistry

Dental surgery

Dental Implants
Maxillofacial Surgery

Dental prosthetics

Cosmetic dentistry

Professional Dental Hygiene

Periodontics
Orthodontic dentistry
Gnathology & TMJ Therapy

Pediatric Dentistry
Dental X-Rays
Search on the site


Popular requests
Teeth whitening
Treatment of caries
Wisdom tooth extraction
Bracket system
Dental veneers
Tooth restoration
Pediatric dentist
Consultation with a dentist-therapist
Search results by: «».
Unfortunately, no results were found for your search: “Pediatric Endocrinologist”, nothing was found.
You may find these links useful:
Clinics "MED-DEO"
пр.Лобановського, 130, Київ, Україна
Temporarily closed
Opening soon
78A, Irpinska St., Kyiv, Ukraine
Temporarily closed
Opening soon
32A, Heroiv Dnipra St., Kyiv, Ukraine
Temporarily closed
Opening soon
9B, Yevhena Chykalenko St. (Pushkinska), Kyiv, Ukraine
Temporarily closed
Opening soon
Services
DentistryGeneral Dentistry
Dental surgery
Dental Implants
Maxillofacial Surgery
Dental prosthetics
Cosmetic dentistry
Professional Dental Hygiene
Periodontics
Orthodontic dentistry
Gnathology & TMJ Therapy
Pediatric Dentistry
Dental X-Rays

")
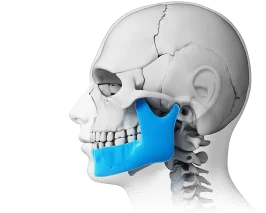
Distal bite is a malocclusion in which the upper jaw is noticeably protruded forward relative to the lower jaw. It is one of the most common orthodontic conditions, affecting approximately 20–30% of patients. Importantly, this is not merely an aesthetic concern — distal bite can affect chewing, breathing, and temporomandibular joint function, combining both aesthetic and functional challenges.
What Is Distal Bite (Prognathia)?
Distal bite, or prognathia, is a condition in which the upper jaw is significantly protruded forward in relation to the lower jaw, resulting in improper occlusion. Under normal circumstances, the upper front teeth only slightly overlap the lower ones, ensuring proper chewing, clear speech, and harmonious facial features.

When a distal bite develops, the lower jaw appears to be shifted backward while the upper teeth protrude excessively. In dentistry, this jaw relationship is referred to as distal occlusion.
Externally, this condition is often recognizable by characteristic signs such as the upper lip projecting forward (physiological prognathia), the chin appearing small or receding, and the facial profile becoming more convex — sometimes described as a “bird face.”
It is important to understand that a slight protrusion of the upper jaw in infants is entirely normal and is associated with developmental processes and the sucking reflex. As the child grows, the jaws typically align. However, if this jaw deformity persists into adolescence or adulthood, it is considered a pathology and should be evaluated by an orthodontist.
Sagittal Gap in Distal Bite
The sagittal gap is the horizontal distance between the upper and lower front teeth — in other words, how far the upper teeth “protrude” in front of the lower ones. Under normal conditions, this distance is approximately 2–3 mm. A measurement exceeding 5–7 mm is considered indicative of a distal bite.
The orthodontist measures this distance during examination or using dental arch models. The measurement helps determine the severity of the malocclusion and identify the appropriate course of treatment. The larger the sagittal gap, the greater the associated problems: difficulty biting food, accelerated tooth overload, increased risk of dental trauma, and occasional changes in sound articulation. This is precisely why this measurement is critical for assessing the severity of the bite.
Causes of Distal Bite
Distal bite develops under the influence of various factors that disrupt normal jaw growth and proper dental occlusion. It most commonly results from a combination of hereditary characteristics and external influences acting during childhood. Understanding the causes of distal bite helps enable timely prevention and the selection of effective treatment.
Genetic Predisposition and Heredity
If parents have prognathia (distal occlusion) or other bite disorders, the risk of a child developing a distal bite increases by approximately 60–70%. Genetic factors may determine the size and shape of the jaws, the relationship between the upper and lower jaw, the rate of facial skeletal bone growth, and the characteristics of dental arch development. This is why distal bite sometimes occurs even without any apparent external causes.

Underdeveloped Lower Jaw: Formation Mechanism
One of the key causes is underdevelopment of the lower jaw — a condition known as micrognathia. In such cases, the upper jaw may be of normal size but appears protruded because the lower jaw is lagging in growth, often referred to as a narrow jaw.
The main factors inhibiting lower jaw development include calcium and vitamin D deficiency, rickets in childhood, hormonal and endocrine disorders, and insufficient chewing load due to a predominantly soft-food diet. The jaws grow most actively during the periods of 6–12 years and 13–16 years, making these the timeframes when negative factors have the greatest influence on distal bite formation.
Harmful Habits in Childhood
The most common habits contributing to the development of distal bite are thumb sucking, prolonged use of pacifiers or bottles, and biting the lips and cheeks. To reduce the risk of malocclusion, it is recommended that pacifier use be discontinued before 1.5 years of age.
Mouth Breathing and Nasal Airway Obstruction
During mouth breathing, the tongue position changes, disrupting the muscle balance and the growth of the lower jaw. Common causes of mouth breathing include adenoids, chronic rhinitis, sinusitis, and a deviated nasal septum. Resolving breathing problems is essential to the effective treatment of distal bite.
Additional Risk Factors
Further contributing causes include premature loss of deciduous teeth, dysfunction of the masticatory muscles, a habitual tendency to sleep on one side, and jaw injuries sustained during childhood.
Symptoms and Signs of Distal Bite
Distal bite can be identified both by the external appearance of the face (the “bird face”) and by the manner in which the teeth and jaws function. This anomaly affects not only aesthetics but also chewing, speech, and breathing. The signs can broadly be divided into external and functional categories.
External Signs (Bird Face)
In distal bite, the proportions of the face change, particularly in its lower portion, and this is most clearly visible in profile. Typical external manifestations include a noticeably protruding upper jaw, a curved or tense-looking upper lip, a chin that appears small or retrognathic, a more convex facial profile, a pronounced chin fold, lips that may not fully close with the mouth often slightly open, and in some cases a visible facial asymmetry. Changes in appearance are most often what prompts a person to consult an orthodontist.
Functional Disorders
Distal bite, or prognathia, affects everyday activities related to jaw function. Due to improper dental occlusion, a range of practical difficulties arise. The most common functional manifestations include difficulty biting hard food with the front teeth, chewing predominantly on one side, possible swallowing difficulties, altered articulation of certain sounds, impaired nasal breathing with possible snoring, and rapid jaw fatigue during chewing. Over time, these functional impairments can worsen, making early detection of distal bite an important step in preventing more serious complications in the future.
Types and Classification of Distal Bite
Distal bite presents differently in each individual, and its classification helps determine the most appropriate corrective approach. The classification takes into account which teeth or jaws are displaced and the degree of severity of the problem.
Angle Classification (Class II)
According to Angle’s classification system, distal bite is assessed based on the position of the first molars and the anterior teeth. Class II, Division 1 is characterized by upper front teeth that protrude and are tipped forward. This typically results in significant overlapping of the lower incisors and a protruding facial profile. Class II, Division 2 involves the entire upper jaw protruding forward while the front teeth are slightly tipped backward. The profile changes less dramatically, but the bite remains abnormal.
In simplified terms, Division 1 involves “protruding teeth,” while Division 2 involves “a protruding jaw.” This classification helps the orthodontist select the appropriate treatment method.
Classification by Severity
Another important criterion is the size of the sagittal gap — the distance between the upper and lower front teeth. A mild bite corresponds to a gap of 3–5 mm, a moderate bite to 5–9 mm, and a severe bite to more than 9–10 mm. The degree of severity determines the treatment approach. A mild case can often be corrected with braces or aligners, while moderate and severe cases frequently require a comprehensive approach involving orthopedic appliances and, in some cases, surgical intervention.
Health Consequences of Distal Bite
Distal bite is not merely a cosmetic issue. If left untreated, it can seriously affect the teeth, jaws, breathing, and even psychological well-being.
Impaired Chewing Function
With a malocclusion, the teeth do not function evenly. As a result, tooth enamel wears down more quickly, the risk of cavities increases, food is more difficult to chew properly which affects digestion, and individual teeth and jaw muscles become overloaded. In distal bite, teeth are often positioned too closely together and may overlap. This makes it difficult to clean the proximal tooth surfaces with a toothbrush, and plaque accumulates easily in such areas, increasing the risk of hidden caries.
Breathing and ENT Problems
Distal bite can narrow the airway, forcing the individual to breathe through the mouth. This can lead to chronic rhinitis, snoring and even sleep apnea, and frequent colds due to reduced natural nasal defense mechanisms. Correcting the bite improves breathing and reduces the risk of ENT complications.
Facial Profile Deformation
Over time, the bite can affect the appearance of the face, causing the corners of the mouth to droop, deepening nasolabial folds, and disrupting facial harmony. These changes can reduce self-esteem and negatively impact psychological well-being.
Temporomandibular Joint (TMJ) Overload
The TMJ is the joint that allows the mouth to open and close. In distal bite, it frequently functions improperly, which manifests as pain in the jaw, temples, and ears, clicking or grinding sounds when opening the mouth, limited jaw mobility, and headaches or migraines. Without treatment, there is a heightened risk of developing TMJ arthrosis. This is why correcting the bite must address not only the teeth but also the joint itself.
Gum and Periodontal Problems
Improper tooth positioning makes oral hygiene more difficult to maintain. The consequences include an increased risk of gingivitis and periodontitis, gum recession, and a higher likelihood of early tooth loss. Correcting the distal bite helps preserve the health of teeth and gums, improves appearance, and reduces the risk of serious complications in the future.
Diagnosis of Distal Bite
To identify a distal bite and develop a treatment plan, the orthodontist conducts a comprehensive examination, assessing the external appearance of the face, the teeth and jaws, and their function.
How Diagnosis Is Conducted
The diagnostic process begins with an external examination and bite analysis, which often reveals a narrow jaw, followed by a functional assessment of jaw movement. Instrumental methods include OPG (orthopantomogram) — a panoramic radiograph of the jaws; TRG (teleradiograph) — a lateral cephalometric X-ray; cephalometric analysis involving precise measurements of angles and distances; 3D scanning to create a digital model of the teeth and jaws; and facial photometry to evaluate proportions and aesthetics. Comprehensive diagnostics allow the clinician to accurately understand the problem and select the optimal treatment.
Treatment Methods for Distal Bite
The choice of treatment depends on the patient’s age and the complexity of the malocclusion. The earlier treatment begins, the easier the correction process.
Treatment in Children (Ages 6–12)
During the primary and mixed dentition period, correction is most effective. Removable plates are used to align the teeth and form the correct bite. Myofunctional trainers such as Myobrace and the LM Activator stimulate lower jaw growth and help eliminate harmful oral habits. Functional appliances — including the Twin Block, Fränkel appliance, and Herbst appliance — correct the bite and normalize muscle tone. The Delaire face mask may be used in cases of pronounced skeletal discrepancies.
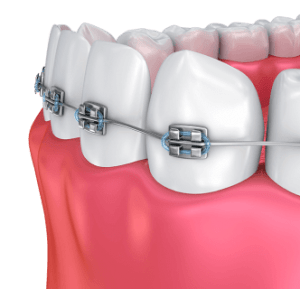
Braces for Adolescents and Adults
Orthodontic treatment with fixed appliances is applied from ages 12–14 onward. Metal braces offer high effectiveness and affordability. Ceramic and sapphire braces provide a more aesthetic appearance. Lingual braces are placed on the inner surface of the teeth, making them invisible from the outside. Aligners (clear removable trays) are a comfortable option but are not suitable for all cases. Treatment typically lasts 1.5 to 3 years, after which retainer wear is mandatory to maintain the result.
Surgical Treatment
Surgical intervention is necessary for severe skeletal forms of distal bite in adult patients. The procedure involves osteotomy of the lower and/or upper jaw. The treatment sequence consists of preparatory orthodontic treatment with braces, followed by surgery, and then post-operative orthodontics. The result is a harmonious facial profile and improved occlusal function.
Comprehensive Therapy
A combined approach integrating orthodontic treatment with myofunctional therapy includes exercises for the tongue, lips, and cheeks; breathing exercises; speech therapy for articulation disorders; and correction of harmful habits. This approach helps not only to straighten the teeth but also to normalize jaw function, muscular balance, and breathing patterns.
Prevention of Distal Bite
To prevent the development of prognathia in children, it is important to take preventive measures from an early age. Pacifier use should be discontinued by 1 to 1.5 years of age. Harmful habits such as thumb sucking and lip biting should be actively corrected. Proper chewing habits should be encouraged by introducing hard foods such as apples, carrots, nuts, and rusks into the child’s diet. Nasal breathing should be normalized through timely treatment of ENT conditions, including adenoid removal when necessary. Regular check-ups with a pediatric dentist and orthodontist should begin from ages 3–4. Preventive trainers may be recommended by the physician to ensure proper jaw function. These straightforward measures help the child develop a correct bite and significantly reduce the risk of complex treatment in the future.
Frequently Asked Questions (FAQ)
Can distal bite be corrected in adulthood?
Yes, it can, but treatment is generally longer and more complex, and surgery combined with braces may be required.
How long must braces be worn for distal bite?
Treatment typically lasts from 1.5 to 3 years, after which retainer wear is mandatory to maintain the result.
What happens if distal bite is left untreated?
Potential consequences include problems with chewing, speech, and breathing; accelerated tooth wear; changes in facial profile; and overloading of the temporomandibular joints.
What is the sagittal gap in distal bite?
It is the horizontal distance between the upper and lower front teeth. The normal range is 2–3 mm; in distal bite, it may measure 5–7 mm or more.
The article was written by Natalia Shmarchuk, a pediatric dentist, orthodontist, and restorative dentist.






Make an appointment
You can make an appointment by filling out the application form on the website, as well as using instant messengers:
Make an appointment
You can make an appointment by filling out the application form on the website, as well as using instant messengers:


Make an appointment easily using chatbots:
Also, call the numbers:
Modern dentistry and medical centre "MED-DEO"
Choose a clinic whose location is more convenient for you.
Kyiv, Holosiivska/Demiivska metro station
130 Lobanovskoho Avenue
")
")
")
")
Working hours:
Mon - Sun: 8:00 AM - 9:00 PM
No days off!
Call the numbers:
How to get to us? Create a route
Create a route
Kyiv, Akademistechko metro station
78A, Irpinska str.




Working hours:
Mon-Sun: 8.00-21.00
Without days off!
Call the numbers:
How to get to us?
Create a route
Kyiv, Heroiv Dnipra metro station
32A, Heroiv Dnipra str.



Working hours:
Mon-Sun: 8.00-21.00
Without days off!
Call the numbers:
How to get to us?
Create a route
Kyiv, Teatralna metro station
9B, E. Chykalenko (Pushkinska) str.




Working hours:
Mon-Sat: 8.00 - 21.00. Sun: by appointment.
Without days off!
Call the numbers:
How to get to us?
Create a route
Відгук від клієнта
0:00
0:00

Your email will not be published on the site.