Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Special offer! Comprehensive professional teeth cleaning for only 1699 UAH.
Sign up
 (044) 394 90 94
(044) 394 90 94
Sign up
(044) 394 90 94
Doctors



 Prices
Blog
Contacts
Prices
Blog
Contacts
пр.Лобановського, 130, Київ, Україна
Temporarily closed
Opening soon
78A, Irpinska St., Kyiv, Ukraine
Temporarily closed
Opening soon
32A, Heroiv Dnipra St., Kyiv, Ukraine
Temporarily closed
Opening soon
9B, Yevhena Chykalenko St. (Pushkinska), Kyiv, Ukraine
Temporarily closed
Opening soon
(044) 394 90 94
Back
Dentistry

General Dentistry

Dental surgery

Dental Implants
Maxillofacial Surgery

Dental prosthetics

Cosmetic dentistry

Professional Dental Hygiene

Periodontics
Orthodontic dentistry
Gnathology & TMJ Therapy

Pediatric Dentistry
Dental X-Rays
Search on the site


Popular requests
Teeth whitening
Treatment of caries
Wisdom tooth extraction
Bracket system
Dental veneers
Tooth restoration
Pediatric dentist
Consultation with a dentist-therapist
Search results by: «».
Unfortunately, no results were found for your search: “Pediatric Endocrinologist”, nothing was found.
You may find these links useful:
Clinics "MED-DEO"
пр.Лобановського, 130, Київ, Україна
Temporarily closed
Opening soon
78A, Irpinska St., Kyiv, Ukraine
Temporarily closed
Opening soon
32A, Heroiv Dnipra St., Kyiv, Ukraine
Temporarily closed
Opening soon
9B, Yevhena Chykalenko St. (Pushkinska), Kyiv, Ukraine
Temporarily closed
Opening soon
Services
DentistryGeneral Dentistry
Dental surgery
Dental Implants
Maxillofacial Surgery
Dental prosthetics
Cosmetic dentistry
Professional Dental Hygiene
Periodontics
Orthodontic dentistry
Gnathology & TMJ Therapy
Pediatric Dentistry
Dental X-Rays
")

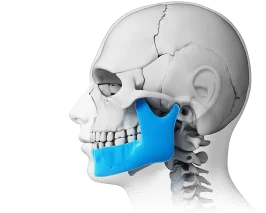
Abfraction is a non-carious lesion affecting the hard tissues of teeth. It develops without bacterial involvement or decay, specifically in the cervical area of the tooth—the region just before the tooth’s neck, directly adjacent to the gums. In other words, where the tooth transitions into the gum tissue.
Visually, abfraction appears as a V-shaped notch at the gum line. Think of it as a chip or “step” near the tooth’s neck with a characteristic wedge shape. This condition affects approximately 20-30% of middle-aged and elderly individuals. Without treatment, it tends to progress over time.
What Is Abfraction?
Abfraction is a non-carious enamel lesion that affects both the enamel and dentin (the inner layer beneath the enamel) in the cervical region. These wedge-shaped defects develop due to both mechanical and functional factors—for instance, prolonged use of an overly stiff toothbrush or improper chewing forces on the teeth. As a result, the enamel either wears away or develops cracks.
The term “abfraction” comes from the Latin words “ab” (away from) and “fractio” (breaking), literally meaning “breaking away of particles” (enamel loss). The condition gets its name from its characteristic V-shaped form, which essentially exposes the cervical area where the tooth meets the gum. This region has the thinnest, most vulnerable enamel and bears significant stress.
: Causes, Stages, and Modern Treatment Options 1")
The anatomical vulnerability lies in the cervical zone’s minimal enamel thickness, which concentrates substantial chewing forces and ultimately leads to abfraction. The formation mechanism works like this: excessive pressure creates micro-cracks in the enamel → mineral loss occurs (demineralization) → the defect itself forms.
Abfraction differs fundamentally from cavities. Unlike decay, it’s not caused by bacteria. With cavities, enamel destruction happens due to acids produced by bacteria in plaque or tartar. With abfraction, bacteria play no role whatsoever.
Abfraction vs. Erosion and Abrasion: How to Tell Them Apart
Abfraction is often confused with other types of non-carious tooth wear, such as erosion and abrasion. However, wedge-shaped defects have somewhat different causes and symptoms. Let’s break down these distinctions.
Here’s a handy comparison table: Abfraction vs. Erosion and Abrasion
| Criteria | Abfraction | Enamel Erosion | Dental Abrasion |
|---|---|---|---|
| Location | Cervical area – only near gums | Any tooth surface | Chewing surface, incisal edge |
| Defect shape | V-shaped, well-defined | Rounded, saucer-shaped | Uniform enamel wear |
| Primary cause | Mechanical overload | Chemical action of acids (from food or stomach) | Friction from excessive chewing, bruxism |
| Progression rate | Slow but steady | Often rapid | Gradual |
| Typical symptoms | Sensitivity, cold-induced pain | Increased sensitivity, dull enamel | Altered tooth shape, worn edges |
What Causes Abfraction?
Abfraction has multiple potential causes—it’s a multifactorial condition. Let’s explore the most common culprits behind wedge-shaped defects.
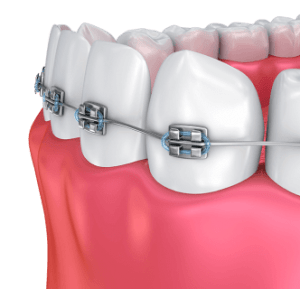
Primary Cause – Malocclusion
The leading cause of abfraction is improper bite alignment. This can involve various malocclusion types—deep bite, crossbite, or open bite.
Malocclusion creates what’s called an occlusal disturbance—incorrect tooth contact. This, in turn, generates occlusal loading: uneven distribution of chewing forces. Teeth receiving excessive pressure develop stress zones in the cervical region. Consequently, enamel micro-cracks form, followed by abfraction.
Additionally, malocclusion can trigger nighttime teeth grinding—bruxism—which is another form of excessive enamel stress.
Interestingly, abfraction often appears symmetrically on corresponding teeth on both the right and left sides due to equal force distribution.
Contributing Factors
Other risk factors for abfraction include:
Aggressive brushing – exclusively horizontal brush strokes, excessive pressure, stiff bristles. All of this mechanically wears down weakened cervical enamel and rapidly creates wedge-shaped defects.
Highly abrasive whitening toothpastes – these also significantly damage enamel.
Hormonal and metabolic disorders – these alter mineral metabolism, making enamel brittle.
Gastrointestinal conditions – high acidity, gastroesophageal reflux disease (GERD), etc. Stomach acid typically enters the mouth and further demineralizes enamel.
Mineral and vitamin deficiencies – particularly calcium, phosphorus, and vitamin D.
Age-related changes – natural enamel weakening after age 40.
Stages of Development and Symptoms
Abfraction progresses through distinct stages with corresponding symptoms. Classification is based on lesion depth: initial, superficial, moderate, and deep stages.
Keep in mind that this defect is progressive in nature—without proper treatment, it only deepens. The overall development timeline, from initial to deep stage, typically spans 5-15 years.
Below you’ll find before-and-after photos of abfraction for reference. These images are often taken at dental clinics to help patients visualize the actual problem. The photos clearly show the stage of damage, which helps determine the optimal treatment approach.
: Causes, Stages, and Modern Treatment Options 2")
: Causes, Stages, and Modern Treatment Options 3")
Let’s examine each stage in detail.
Initial Stage
Early-stage abfraction has these characteristics:
Features – barely noticeable enamel thinning in the cervical zone, depression less than 0.1 mm, defect virtually invisible to the naked eye.
Symptoms – usually absent or brief, minor sensitivity to cold.
Diagnosis – detected only through careful examination under magnification or when the tooth surface is dried (which reveals structural changes in the enamel).
Progression is easiest to halt at this stage.
Superficial Stage
Surface-level abfraction shows these characteristics:
Features – clearly defined small notch, depth 0.1-0.2 mm, length up to 3-3.5 mm. The defect takes on a shallow wedge shape.
Symptoms – periodic moderate tooth sensitivity to cold, possible pain from acidic foods, and reaction to sweets, especially during brushing or when consuming cold beverages.
Visual signs – yellowing may appear near the gums due to dentin showing through the thinned enamel.
Moderate Stage
Mid-stage abfraction presents these features:
Characteristics – depression has a quite distinct wedge shape at approximately 45-degree angle, depth now 0.2-0.3 mm and length 3.5-4 mm. The lesion now extends into the dentin.
Symptoms – pronounced tooth hypersensitivity to temperature, chemical, and mechanical stimuli. Also discomfort during brushing and significant pain from acidic foods.
Aesthetic changes – yellow or brown dentin beneath the enamel, clearly visible in the notch. The defect becomes quite noticeable during conversation and smiling.
Deep Stage
Advanced abfraction has these characteristics:
Features – obvious deep V-shaped defect with sharp edges, depth exceeding 0.3-0.5 mm (sometimes up to 1 mm), length 4-5 mm. Possible involvement near the pulp chamber (inside the tooth, where nerves and blood vessels are located).
Symptoms – constant severe sensitivity to any stimuli, sharp pain on contact, and brushing these affected teeth becomes nearly impossible.
Complication risks – possible pulpitis (nerve inflammation) and crown fracture in the weakened area.
Diagnosing Abfraction
Timely and accurate diagnosis of abfraction is essential to prevent further progression. Let’s look at detection methods used during dental appointments.
Visual Examination
The primary diagnostic method is visual inspection. The dentist carefully examines the cervical area under bright specialized lighting. To enhance visual assessment accuracy, magnification is used—for example, viewing enlarged defect images on a screen. Additionally, tooth surface drying and probing help detect even initial enamel changes.
Additional Tests
Supplementary diagnostic procedures typically include:
Radiography – to assess lesion depth and proximity to the pulp chamber (tooth nerves). Performed at deep stages.
Orthodontic consultation – essential for comprehensive bite evaluation as the primary cause. Also includes occlusion analysis (tooth contact) and identification of excessive load zones.
Treating Abfraction
Treating abfraction requires a comprehensive approach. The most effective strategy combines addressing the root cause and restoring tooth form and function. Crucially, eliminating the underlying cause is paramount. You need not just cosmetically fill the enamel gap but also work on correcting the bite, adjusting occlusion, and reducing overall tooth stress.
Let’s explore various treatment methods for abfraction in detail.
Eliminating the Cause – The Foundation of Successful Treatment
When abfraction is present, treatment must first target the underlying problem. Cosmetic restoration without addressing the root cause will simply be ineffective. Residual excessive loading will cause new defects on other teeth, and fillings will constantly fall out.
The most common cause of abfraction is malocclusion. Therefore, bite correction is mandatory. This involves orthodontic treatment (braces, aligners) and a night guard for bruxism (to prevent wear from grinding). Selective grinding of teeth may be performed if necessary.
Correcting home hygiene practices is also crucial—specifically, learning proper brushing technique (primarily vertical strokes with gentle pressure), switching from stiff to soft bristles, and avoiding abrasive pastes.
Other steps to eliminate root causes include treating systemic conditions—most commonly normalizing GI function, correcting hormonal imbalances, and taking vitamin-mineral supplements.
Conservative Treatment for Initial Stage
Conservative treatment aims to halt progression of the problem—this is the phase when you can still stop wedge expansion without filling (in early stages).
Conservative treatment methods include:
Remineralization therapy – applying calcium and phosphorus preparations, plus fluoride treatments (Tooth Mousse, Fluoridex). Performed in courses specifically for long-term enamel strengthening.
Professional applications at the dental office – fluoride varnish or gel to reduce sensitivity and strengthen enamel structure. Done once or periodically, but not in courses.
Filling Abfraction Defects
Filling becomes necessary when the defect becomes noticeable and significant tooth sensitivity develops. This is typically at the dentist’s recommendation, but fillings for abfraction have unique challenges. The difficulty lies in the absence of supporting walls (firm tooth edges), with frequent risk of filling loss. Therefore, perfect moisture isolation and careful shaping are essential—so the filling stays secure in the cervical zone without creating additional enamel pressure.
Flowable composite is often used for filling abfraction. Its enhanced flowability allows excellent adaptation precisely in the cervical zone, effectively filling the V-shaped notch and reducing the risk of voids around it.
Prosthetic Treatment for Deep Defects
Prosthetic treatment is required when the defect is deep and crown fracture risk emerges, or when filling won’t provide reliable long-term tooth protection. In such advanced cases, recommendations include:
Ceramic veneers – thin ceramic overlays on the front tooth surface that cover the defect and restore aesthetics. Veneer placement is indicated mainly for front teeth and multiple defects.
Crowns – full tooth coverage, indicated for deep defects with natural crown fracture risk. Artificial crowns provide maximum tooth protection as prosthetic treatment.
Prosthetic treatment advantages: longevity (up to 10-15 years), excellent aesthetics, and complete restoration of tooth function.
Minor drawbacks: tooth preparation necessary and higher cost compared to filling.
Can You Stop Abfraction Without Treatment?
Many patients wonder whether abfraction can be stopped without treatment. Let’s be clear upfront—spontaneous reversal doesn’t happen; enamel doesn’t regrow. But let’s examine how to at least halt progression if abfraction is already present.
Here’s the breakdown:
: Causes, Stages, and Modern Treatment Options 4")
At the initial stage: progression can be slowed or nearly stopped with mandatory bite correction (i.e., eliminating the root cause). Also effective: intensive remineralization, proper home hygiene, and regular dental monitoring.
At superficial and moderate stages: without filling, the defect will continue deepening even with perfect prevention. Typical progression rate: 0.1-0.3 mm over 2-5 years, depending on risk factors.
At the deep stage: only prosthetic treatment (crowns or veneers) will help. Without this, there’s high risk of complications like pulpitis or even tooth fracture.
REMEMBER: Prevention is effective only at defect onset or after filling to prevent new defects. Don’t put it off!
Preventing Abfraction
When dealing with abfraction, preventive measures are crucial to stop progression. There are also preventive steps to avoid its initial development. In both cases, a comprehensive approach is essential.
Let’s look at various prevention methods for abfraction.
Bite Correction and Load Control
As the primary preventive measure, this involves timely correction of malocclusion in childhood/adolescence or adulthood. Treating bruxism is also important, as it’s usually caused by malocclusion too. This involves making and wearing a special night guard to protect teeth from grinding. Equally important: even distribution of chewing forces—chew food on both sides and promptly address missing teeth with prosthetics.
Proper Home Hygiene
As a preventive measure, proper home hygiene is often undervalued. Yet it’s highly significant and includes:
Correct brushing technique – vertical brush strokes from gum to tooth edge (sweeping motion). Categorically avoid horizontal motions (sawing action). Brush for at least 2-3 minutes.
Choosing the right products – use soft or medium-bristle toothbrushes (never stiff). Select low-abrasiveness toothpastes (RDA up to 70), for example, sensitivity toothpastes with calcium and fluoride. Avoid whitening toothpastes with high abrasiveness.
Using supplementary aids – use dental floss daily and fluoride rinses when possible.
General Recommendations
Beyond the preventive methods listed above, these general recommendations are important:
Regular dental visits – checkups every 6 months for early detection of initial stages, even when nothing’s bothering you.
Professional cleaning – dental cleaning 1-2 times yearly to remove hard deposits (plaque and tartar).
Balanced nutrition – adequate calcium intake (dairy products), vitamin D, phosphorus, and limiting acidic beverages (juices and carbonated drinks).
Treating concurrent conditions – normalizing GI function (especially acidity levels) and correcting hormonal imbalances.
Breaking harmful habits – don’t chew hard objects (nuts, ice), don’t bite nails, don’t open bottles with teeth.
Frequently Asked Questions (FAQ)
What is abfraction in simple terms?
In plain English, abfraction is a small notch in the enamel right at the gum line. It has a V-shape and develops from mechanical stress, not cavities.
Can abfraction be treated without filling?
You can’t cure abfraction without filling. However, you can slow or nearly stop its progression—most often at the initial stage. This requires enamel remineralization and bite correction.
Why do fillings fall out of abfraction defects?
Fillings in abfraction defects typically fall out due to lack of support structure and constant excessive chewing forces on this cervical tooth area.
How do you stop abfraction development at the initial stage?
You can halt early-stage abfraction development. Eliminate the root cause of its formation, then strengthen enamel and maintain proper home hygiene.
Does abfraction hurt?
Abfraction doesn’t hurt at the initial stage. At moderate or deep stages, the tooth may hurt and shows significant sensitivity to temperature or chemical irritants.
Article authored by Dr. Maria Lukyanyuk, DDS – Orthodontist and Gnathologist






Make an appointment
You can make an appointment by filling out the application form on the website, as well as using instant messengers:
Make an appointment
You can make an appointment by filling out the application form on the website, as well as using instant messengers:


Make an appointment easily using chatbots:
Also, call the numbers:
Modern dentistry and medical centre "MED-DEO"
Choose a clinic whose location is more convenient for you.
Kyiv, Holosiivska/Demiivska metro station
130 Lobanovskoho Avenue
")
")
")
")
Working hours:
Mon - Sun: 8:00 AM - 9:00 PM
No days off!
Call the numbers:
How to get to us? Create a route
Create a route
Kyiv, Akademistechko metro station
78A, Irpinska str.




Working hours:
Mon-Sun: 8.00-21.00
Without days off!
Call the numbers:
How to get to us?
Create a route
Kyiv, Heroiv Dnipra metro station
32A, Heroiv Dnipra str.



Working hours:
Mon-Sun: 8.00-21.00
Without days off!
Call the numbers:
How to get to us?
Create a route
Kyiv, Teatralna metro station
9B, E. Chykalenko (Pushkinska) str.




Working hours:
Mon-Sat: 8.00 - 21.00. Sun: by appointment.
Without days off!
Call the numbers:
How to get to us?
Create a route
Відгук від клієнта
0:00
0:00

Your email will not be published on the site.